PUBLIC SERVICE ARTICLE
Types of Self-Esteem and Sound Mental Health
Could There Be a “Master Personality Mechanism”?
Joseph William Ferrara, EdD, LMHC
www.soundmentalhealth.com
INTRODUCTION
Hidden deep in our common shadowy, dysfunctional, threatening unconscious, paired-associative human mind are living many repressed, classified secret dreams, taboo wishes, forbidden desires and antisocial urges (9, 12, 16 & 23). Our socialized state of awareness and degree of both covert and overt or multiaxial self-esteem have to hourly cope with these frightening urges, wishes and dreams as our electrochemical brain through varied social sensory-channel experiences and level and range of awareness becomes a cogitating human mind, they are our past and they are our future (1, 5, 11 & 26). These unthinkable, unspeakable and socially unacceptable primal wishes, desires and urges are automatic, incessant and involuntary stressful demands on our socialized state of awareness and its Life-Giving Multiaxial Self-Evaluated Mechanism or covert and over self-esteem housed in our mammalian human body (7, 11, 13 & 14).
The oversimplification and overuse of self-esteem has led to both gross misunderstanding and underestimating its life-giving, nurturing and/or lethal paired-associative antecedents and subsequent desirable or fatal consequences, a tragedy (4, 7, 10, 12, 16 & 26). Nevertheless:
| I. | Do the different psychogenic psychiatric diagnostic disorders (DSM-5-TR, 2022) have a common denominator which can fit into a single treatment program, irrespective of patients’ differential psychiatric intake complaints or symptoms? | |
| II. | Does a mental health counselor/psychotherapist need separate treatment theories and programs for individual, marriage, family and group psychotherapy when treating anxiety/anger, depression/elation, schizophrenia, suicidal/homicidal obsessions, eating disorders, dysfunctional relationships, alcohol/drug compulsions, dependency/subjugation, passivity/aggression and related symptoms? | |
| III. | Which psychotherapy theory is best or is there a common denominator among the major established theories which fit into a single treatment program? | |
| IV. | As the pituitary “master gland” on a physical level allegedly asserts “various regulatory and controlling dominance of our endocrine system”, could there be on a psychological level a “master personality mechanism” which regulates and controls human covert personality structure and subsequent overt behavior? | |
| V. | How might the context, content, structure and function of the multiaxial or covert and overt self-evaluative mechanism become rational, healthy, wholesome and life-giving? | |
| VI. | Can such a differential treatment program bring success, happiness and a prosperous, loving, family, interpersonal and social life? |
RELEVANT THEORY AND RESEARCH
To answer the foregoing questions, a historical, conceptual and summary perusal of the relevant bibliographical research body of established clinical hypnosis (18 & 27), psychopathology (2, 3, 20, & 22), psychotherapy (4, 8, 12, 15, 20, 22 & 23), personality (10, 12, 18, 19, 20 & 25) and learning theorists (8, 17 & 28) essentially designate that regardless of its type, our core degree of multiaxial or covert and overt degrees of self-esteem (5, 16, 26 & 29) tends to act as the “tap root”, “heart” or “backbone” and thus perhaps a “master personality mechanism” which regulates human choices and subsequent outcomes which determines life’s desirable or undesirable consequences. With every beat of our heart, breath and step we take in our social order on planet earth, our invisible multiaxial or covert and overt degrees of the self-evaluative mechanism is involuntarily, silently passing our introjected and imprinted value-judgment on us which in turn becomes our identity, self-concept and self-actualizing destiny(11, 16 & 29). In his 1954 publication, The Psychiatric Interview, H. S. Sullivan, erstwhile psychiatrist at Walter Reed General Hospital, declared “we must find a direct way to treat the schizophrenics’ self-esteem”. Most commonly, self-esteem is obsessively contingent upon the lethal multiaxial or covert and overt interactive and interactive performance of the following cluster of symptoms or conditions, i.e., common everyday but lethal, conditional/dependent sources of multiaxial or covert and overt degrees of self-esteem (21).
Common Conditional or Varied Sources of Interactive Multiaxial or Covert and Overt Self-Actualizing/Realized Self-Esteem:
| Axis I. | Body type/image, libido/sex drive/impulsivity, gender, age, appearance/beauty/handsomeness and race/nationality. | |
| Axis II. | Fears, threats, intimidation/bullying, security/insecurity, vulnerability/invulnerability and punishment/rewards. | |
| Axis III. | Attention, compulsively pleasing others, approval/disapproval, acceptance/rejection and authority/power. | |
| Axis IV. | Insults, antagonism, pride/humiliation, aggression, anti-social/criminal behaviors. | |
| Axis V. | Family habits, social rituals, political customs, religious laws/beliefs and/or civic group(s)’ traditions and membership(s). | |
| Axis VI. | Intelligence level and range, education/grades, feelings of adequacy/inadequacy and achievements/failure, sports/athletics and publicity. | |
| Axis VII. | Employment/unemployment, occupation/profession/titles and fame/fortune. | |
| Axis VIII. | Income, possessions/assets, recognition/popularity and awards. |
Consequently, the most important value-judgment we will ever make is the value and worth our interactive conscience component on the unconscious level of our self-evaluative mechanism places on ourselves and subsequently others (12, 16, 25 & 26). How we regard and accept ourselves defines how we value and treat our personhood and others which expresses our operational sense of worth/importance, belongingness, adequacy/mastery, usefulness and future happiness. Our level and range of awareness and degree of both multiaxial or covert and overt self-esteem acts as the life-giving origin and direction setter for what we think, feel, say and do. We communicate accepting and/or rejecting thoughts and affect/feelings with words towards and about ourselves and others both covertly and overtly. Through our sensory channels both our paired-associative unconscious mind and the social DNA or context and content of our background involuntarily actuates Imax mental images which in turn generates needs, wishes, feelings and desires. These Imax images are then automatically, involuntarily transmitted into the electrochemical neuron structure of the cells in the tissues of our organic brain. Our brain then forms an indelible, obsessive memory of the Imax image or context which, in turn, becomes a compulsive mental/emotional overt habit in our relationships with ourselves and others, dictating our present actualized and future realized life. However, healthy, wholesome unconditional self-actualizing/realized multiaxial or covert and overt self-esteem forms independent and autonomous of the multiaxial or covert and overt, interactive stimulus/response conditioners or everyday sources outlined above.
DEFINITIONS OF TERMS AND TYPES OF SELF-ESTEEM
Self-esteem term and subsequent opinion is discussed far more than any clinical and/or cross validated empirical findings are presented and understood. If there were more of the later and less of the former, multiaxial or covert and overt self-esteem’s profound role in human behavior would be both empirically cross validated and insightfully understood. Multiaxial or covert and overt degrees of self-esteem is not to be confused and equated with narcissism. Thus, for the first time in the clinical history and comprehensive empirical research of the multiaxial or covert and overt self-evaluative mechanism self-esteem, the following terms are both formulated and defined.
This study defines the life-giving multiaxial self-evaluative mechanism or multiaxial self-esteem as both covert/unconsciously hidden and overt/socially manifested and plainly seen degrees of assessed unconscious and conscious thoughts, feelings, and actions towards and about ourselves and others of human worth/importance, acceptance/rejection, feelings of belongingness, usefulness and adequacy/mastery. Figure No. 1. is a single cell outlining and describing the sociogenic, multi-structure and function of the learned multiple cognitive, affective and behavioral growth areas and their traits of our multiaxial or covert and overt self-evaluative mechanism followed by the three (3) sociogenic learned multiaxial or covert and overt self-esteem types.
FIGURE No. 1. – Single Cell of Multiple Growth Areas of Cognitive, Affective and Behavioral Sociogenic Self-Esteem Traits of the Life-Giving Self Evaluative Mechanism
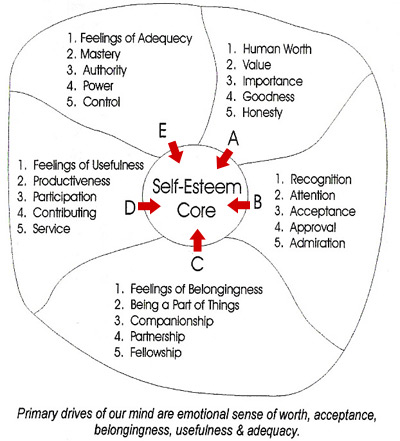
Our every cognition/thought, feeling and act is an effort of our level of awareness, i.e., what we consciously and unconsciously know to gratify our core need to feel worthwhile/valued, important, accepted/belongingness, useful and adequate/capable. Our level of awareness is the clarity with which we perceive both consciously and unconsciously all the factors that affect our lives. Our level of awareness determines the value and worth of our multiaxial, i.e., covert and overt self-esteem which in turn conjointly dictates our choices that set in motion the desirable or undesirable and sometimes lethal consequences we, our loved ones and society will have to cope with. The bipolar terms of drive is motivation and mismotivation which are coexisting, simultaneous perceptual forces passing first through the unconscious prior to any choice, action and subsequence consequences. Motivation is operationally defined as the ability to perceive healthy, wholesome and desirable benefits arising from any proposed, self-actualizing/realized multiaxial choice or action. Mismotivation is defined as any choice which sets in motion unhealthy, undesirable and or painful and sometimes lethal consequences.
Reportedly, the white corpuscles of our immune system is intolerant of pathogens and makes an immediate value-judgment to attack and eliminate without doubt or debate when our bodies are invaded by infection. They protect us against illness and disease. Doubt, tolerance or appeasement of germs by our immune system’s value-judgment would be fatal to our bodies. Thus, as healthy distinguishing blood is life to our bodies, the self-evaluative mechanism is to our personality’s health subsequent rational, healthy prosperous realized life. This clinical research study has operationally identified and defined three (3) major social types of multiaxial or covert and overt self-esteem which make up the composition of the self-evaluative mechanism, i.e., thoughts/feelings towards and about ourselves as being:
| I. | Sociogenic Multiaxial or Covert/Overt Learned Type-A self-esteem: Conditional (most common) | |
| II. | Sociogenic Multiaxial or Covert/Overt Learned Type-B self-esteem: Unconditional (uncommon, Rx. objective) | |
| III. | Sociogenic Multiaxial or Covert/Overt Learned Type-AB self-esteem: Mixed Transactional (experienced during Rx. maturation) |
Self-evaluative mechanism is determined by the attachments or conditions our level of awareness uses as multiaxial, i.e., many and various conditional sources that generate thoughts, feelings and actions/performance which in turn define our human worth/importance, acceptance, belongingness, productiveness and adequacy/mastery. By knowing the interactive covert and overt multiaxial antecedents or variable sources to which our level of awareness formulates and defines our degree of both covert and overt self-esteem, we are able to both successfully treat and predict patient’s differential psychiatric care and subsequent behavior.
STUDY’S INSURANCE COMPLIANCE OF AVAILABLE PSYCHIATRIC PATIENT POPULATION
This heterogenous, longitudinal, circumscribed study was a delimited adolescent and adult, male and female group of 25 timely and geographically available psychiatric patients (DSM-5-TR, 2022) residing in moderate-size Southwest counties in transitory Florida diagnosed, referred and confined by the insurance companies, district courts, human service agencies/psychiatric social workers, physicians, psychologists, psychiatrists and self-referred patients from the general population and public school systems between the chronological ages of 16 and 63 with a mean age of 31 years having a range of 47 years, indicating a positively skewed age distribution. Their Shipley IQ findings were in the middle Average score of 100 level to high Superior score of 128 with a mean level within the Bright-Normal score of 117 and a range of twenty-eight (28) points. Their Shipley Cognitive Quotient, CQ i.e. thought disturbance or impairment test scores were a low score of 69 or profound impairment, a high score of 87 or slight impairment, with a mean test score of 77 or moderate impairment. The range of this set of variable test scores is 18 points. Brain dysfunctioning/impairment or injury was ruled out as designated by intact, completed and accurate Bender Gestalt Test reproductions. Their formal educational levels ranged from high school students, some with earned academic diplomas, to those who earned bachelor and master’s degrees, while their occupations reflected skilled and professional positions. Irrespective of their intake diagnostic dynamics (DSM-5-TR, 2022), these patients symptomatically complained of life-threatening feelings of being unimportant, worthless, rejected, sadness, depressed, useless, anxious, confused/indecisive, angry, suicidal, homicidal, inadequate, inferior and helpless/powerless with meaningful and unfulfilling lives.
Their multiaxial reported acute and/or chronic intake cluster of common problems, complaints or symptoms and psychogenic psychiatric diagnosis were as follows (DSM-III, 1):
| I. | patient reported common intake problems/complaints: alcohol/drug abuse, anger, rage/hostility, suicidal ideation, rejection, compulsions, self-consciousness/withdrawal, passivity, separation/divorce, dependency, poor-judgment, depression, failure, impulsivity, alienation, physical/sexual abuse, anti-social behaviors, daytime and nighttime dreams of suicide, homicide, “pornographic” sex and a “terrorizing hell”. | |
| II. | patient reported intake psychiatric symptoms: poor attention and concentration, confusion and disorganization of thoughts, feelings of worthlessness, insecurity, aggression/hostility/homicidality, indecisiveness, anxiety, sadness/depression/suicidality, hopelessness, uselessness, guilt/judgmental, shame, blame, bland/flat affect, suspiciousness/mistrustfulness, uselessness, inferiority, helpfulness and inadequacy, obsessions/preoccupations, | |
| III. | psychogenic psychiatric intake diagnosis, (DSM-5-TR, 2022): schizophrenia, affective adjustment reaction/bipolar depression, mixed-neurotic, psychoneurotic and character/personality disorders. | |
| IV. | Patients’ intake psychiatric mental/emotional conditions were (DSM-5-TR, 2022): biogenetic/medically unrelated. |
METHOD OF TREATMENT
ASSESSMENT/EVALUATION: All patients were given a treatment pretest and a treatment posttest for both covert and overt degrees of multiaxial self-esteem to determine whether they had sociogenic Type-A or Type-B self-esteem, a Shipley IQ/CQ test for level and range of intellectual/cognitive functioning, House-Tree-Person projective personality test and a Bender Gestalt Visual-Motor test for brain/organic functioning.
MENTAL HEALTH COUNSELING/PSYCHOTHERAPY: These patients received 60 hours of individual, relationship outpatient private practice Psychoanalytic/Rogerian/Behavioral-oriented mental health counseling/psychotherapy with this writer, combined with their trained and monitored use of this writer’s sociogenic multiaxial or covert and overt Type-B degree self-esteem home study materials consisting of three 45-minute fractionalized audio hypnosis tapes treating the cognitive, affective and overt behavioral growth areas of their self-evaluative mechanism on the unconscious level, a 79 page monthly self-testing and progress chart book, 128 page daily study manual and 89 page relationship skills workbook which they studied and filled-out between their weekly one-hour analytic, mental health counseling/therapy sessions.
KINDLY NOTE: Many of these patients stated on their intake form they were “on their way to kill themselves or to kill their boss but saw my practice shingle stating self-esteem management and decided to drop in”. Some had deeply slit one of their wrist while one patient had slit both of his wrists designating acute and chronic agitated depression.
TESTED HYPOTHESIS
Tested Hypothesis were:
| I. | The patients’ post test scores for both covert and overt levels of sociogenic Type-B degree self-esteem would be significantly higher than their intake pretest treatment scores | |
| II. | As pretest covert and overt levels of sociogenic Type-A degree self-esteem decreased, there would be a corresponding increase in both covert and overt Type-B degree self-esteem post test scores producing an elimination of intake psychogenic psychiatric symptomology (DSM-5-TR, 2022). | |
| III. | That as both sociogenic covert and overt Type-B degree self-esteem test scores increased, patients would experience a happier, more successful and productive/prosperous, interpersonal and social loving life. |
TEST FINDINGS/RESULTS
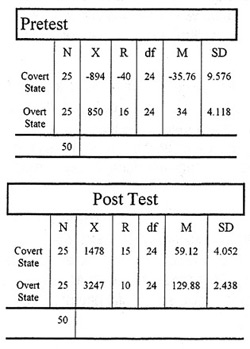
As demonstrated by Table 1, the arithmetical mean test scores for this study were: covert state of sociogenic Type-A degree conditional self-esteem pretest, -35.76 and covert state of sociogenic Type-B degree unconditional self-esteem post test 59.12, yielding (t=4.75, df=24, p<.0001); overt state of sociogenic Type-A degree conditional, multiaxial self-esteem pretest, 34 and overt state sociogenic Type-B degree unconditional self-esteem post test, 129.88, yielding (t=97.84, df=24, p<.0001). These arithmetical numbers strongly suggest that the most significant life-giving value-judgment these patients made was the value, worth and importance they learn to place on the “self” or their self-actualizing/realized unconditional, multiaxial or covert and overt self-esteem, i.e., they perceived the life and death implications of their individual multiaxial or covert and overt self-esteem and took healthy, appropriate and wholesome therapeutic action by keeping their weekly one-hour therapy sessions, utilizing daily the three 45 minute fractionalized audio hypnosis treatment tapes, studying the multiaxial or covert and overt self-esteem manual, relationship skills workbook and monthly self testing and charting of their tested multiaxial or covert and overt self-esteem, which in turn eliminated their self-reported acute and chronic intake psychiatric symptoms (DSM-5-TR, 2022) and any hospitalization.
TABLE 1. Pre and Post Test Measures of Central Value and Variability of Patients Covert and Overt Degree of Sociogenic Type A and Type B Self-Esteem
STUDY’S TESTED CONCLUSIONS
Statistical pre and post hypothesis testing were used in this clinical study to assess the probability that observed, empirical test frequencies within multiaxial or covert and overt degrees of Type A and Type B self-esteem categories significantly different from what is expected under the null hypothesis as simply listed and described below.
| I. | This study identified and defined by direct clinical treatment observation a common denominator associated with the different psychogenic psychiatric diagnostic disorders (DSM-5-TR, 2022) as high levels of both multiaxial covert and overt sociogenic Type-A degree self-esteem, i.e. conditional/provisional human worth/importance, acceptance, belongingness, usefulness and adequacy. | |
| II. | That direct, immediate prescriptive clinical treatment of the core multiple-growth areas of sociogenic Type-A self-esteem eliminated intake symptoms associated with the various psychogenic psychiatric diagnostic disorders (DSM-5-TR, 2022) by increasing life-enhancing unconditional multiaxial covert and overt levels of sociogenic Type-B degree of self-esteem/acceptance. | |
| III. | That the major established relevant body of psychopathology (DSM-5-TR, 2022), psychotherapy and personality/learning theories have as a common denominator the identified and defined core multiple-growth areas of self-esteem as depicted in Figure 1. | |
| IV. | That core degree of multiaxial or covert and overt self-esteem whether sociogenic Type-A or Type-B acts as a master personality construct or conditional or unconditional direction setter which decides one’s choices in determining treatment management and prediction of psychiatric symptoms (DSM-5-TR, 2022). | |
| V. | That these test findings confirm and suggest both covert and overt core levels of sociogenic Type-B multiaxial degree self-esteem as a single, unitary construct for the treatment of psychogenic psychiatric diagnostic disorders (DSM-5-TR, 2022) whether one is receiving individual, marriage, family or group therapy. | |
| VI. | That sociogenic Type-B multiaxial or overt and overt inoculation of self-esteem is essentially what every person needs most, i.e. unconditional/unprovisional human worth/importance, acceptance, feelings of belongingness, usefulness and adequacy/mastery which, in turn, acts as a healthy direction setter and produces a happy, successful and productive/prosperous, loving life. |
PROPOSED LAW OF THE LIFE-GIVING SELF-EVALUATIVE MECHANISM
Pursuant to this clinical study’s significant test findings, the following law of The Life-Giving Multiaxial Self-Evaluative Mechanism is proffered. It is composed of a conscious, subconscious and unconscious state of awareness with multiaxial or interactive degrees of tested both covert and overt self-esteem. Figure No. 2 describes, the amount of stress which the multiaxial or covert and overt self-evaluative mechanism can tolerate is in direct proportion to the various unconscious components and social forces acting upon it. Levels of stress are measured by testing directly the strength of both multiaxial covert and overt degrees of self-esteem. Increased stress beyond the structural limit of both its state of awareness and degrees of multiaxial covert and overt self-esteem will change the function of the Life-Giving Multiaxial Self-Evaluative Mechanism which can be healthy or unhealthy and at times fatal but always constant, permeable and variable as suggested by the test results or findings of this clinical study. Further studies regarding the life-giving traits of the multiaxial or covert and overt types of self-esteem are critically needed.

TESTED CONCLUDING ANALOGIES
This tested mental health counseling/psychotherapeutic study suggests if we choose to learn and put into action the above transforming life-giving traits of multiaxial or covert and overt Type-B Self-Esteem, individuals, our families, nation and our world at large might become more mentally/emotionally rational, accepting and loving as expressed in the below analogies. In both the prevention and elimination of psychiatric symptoms and their disorders (DSM-5-TR, 2022), it is now empirically significant and clinically to recognize the following analogies that healthy multiaxial or covert and overt self-esteem is a critical, tested antecedent to healthy self-acceptance as healthy self-acceptance is a wholesome tested consequence of healthy multiaxial or covert and overt self-esteem which in turn can eliminate noted psychiatric symptoms (DSM-5-TR, 2022).
A. If there is equal human worth/importance, acceptance, a sense of belongingness, usefulness and adequacy/mastery in our personhood or sense of self, there will be equal human worth/importance, truth, honesty and justice in our individual character.
B. If there is equal human worth/importance, truth, honesty and justice in our character, there will be insightful judgment/rational choices, acceptance and harmony in our families.
C. If there is insightful judgment/rational choices, acceptance, honesty and harmony in our families, there will be kindness/genuine respect, justice and a loving order in our nation.
D. If there is kindness/genuine respect, and a loving order of acceptance in our nation, there will be equal worth, dignity, honor, freedom, peace and beauty in a just, honest and rational world, i.e., every person is worthy of genuine consideration and respect.
REFERENCES
-
- Adler, A. The Practice and Theory of Individual Psychology. New York, New York, Harcourt 1927
- American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) Washington D.C., American Psychiatric Press, 2022.
- Cameron, Norman. Personality Development and Psychopathology – A Dynamic Approach. Yale University: Houghton, Mifflin Co., Boston, 1963.
- Carkhuff, Robert R. and Berenson, Bernard G. Beyond Counseling and Therapy. Holt, Rinehart and Winston, Inc., New York, 1967
- Coopersmith, Stanley. The Antecedents of Self-Esteem. San Francisco: W.H. Freeman and Company, 1967.
- Ellis, Albert. Rational Psychotherapy. Journal of General Psychology. Vol 59, pages 35-49, 1958.
- Ellis, Albert. Reason and Emotion in Psychotherapy. New York, New York. Lyle Stuart, 1962.
- Eysenck, H. J. The Effects of Psychotherapy: An Evaluation. Journal of Consulting Psychology, Vol 16, pages 319-324, 1952.
- Ferrara, Joseph W. The Functioning of Immediate Verbal Feedback in Paired Associative Learning with Normals and Retardates, Master’s Degree Thesis – North Texas State University, Denton Texas, 1965
- Ferrara, Joseph W. A Method for Improving Self-Acceptance As a Component in Psychotherapy and Behavior Change, Doctoral Degree Dissertation – The University of Sarasota, Sarasota, Florida, 1977.
- Freud, Sigmund. The Psychopathology of Everyday Life. In the Basic Writings of Sigmund Freud. New York, New York: Random House, 1938.
- Freud, Sigmund. The Standard Edition of the Complete Psychological Works. J. Strachey (Ed). London, England, Hogarth Press, 1953
- Fromm, Erich. The Sane Society. New York: Rinehart, 1955
- Gay, Peter. Freud, A Life For Our Time. First Edition: W.W. Norton & Company, New York, 1988.
- Hall, Calvin S. & Lindzey, Gardner. Theories of Personality. Tenth Printing, John Wiley & Sons, Inc. May 1963.
- Horney, Karen. Our Inner Conflicts. Norton, New York, 1945.
- Hilgard, Ernest R. Theories of Learning. Second Edition, Appleton-Century-Crofts, Inc., 1956.
- Hull, Clark L. Hypnosis and Suggestibility – An Experimental Approach. Yale University: D. Appleton-Century Company, New York, 1933.
- James, William. Principles of Psychology. New York: Hold, 1890.
- Jung, C. G. The Integration of the Personality. (Tr. by S. M. Dill), New York, NY: Holt, 1939.
- Millon, Theodore. Disorders of Personality DSM-III: Axis II. John Wiley & Sons, Inc., 1981.
- Patterson, C.H. Theories of Counseling and Psychotherapy. University of Illinois: Harper & Row Publishers, New York, 1973.
- Rogers, Carl R. Houghton Mifflin Company, Boston, The Riverside Press Cambridge, Boston, MS, 1951
- Rogers, Carl R. and Dymond, R.F. Psychotherapy and Personality Change. Chicago: University of Chicago Press, 1954.
- Strachey, James. The Complete Introductory Lectures on Psychoanalysis, Sigmund Freud. W. W. Norton & Company, New York, N.Y, 1966.
- Sullivan, H.S. The Psychiatric Interview. W.W. Norton & Company, New York, 1954.
- Teitelbaum, Myron. Hypnosis Induction Technics. Fourth Printing, Charles C. Thomas Publisher, Springfield, Illinois, 1978.
- Thorndike, Edward L. Reward and Punishment. Journal of Experimental Psychology, X (April, 1932) 10, 18-29
- Wylie, R.C. The Self-Concept. (Revised Edition) Vol 1. A Review of Methodological Consideration and Measuring Instruments. Lincoln, Nebraska: University of Nebraska Press, 1974.